

A 52-year-old male presented with history of injury to the right hand 1 month ago following which there was pain predominantly along the right middle finger.
Clinical features :
- A 52-year-old male presented with history of injury to the right hand 1 month ago following which there was pain predominantly along the right middle finger.
- On examination, there is swelling and lateral subluxation of the extensor digitorum tendon of third digit on extreme flexion.

EXTENSOR DIGITORUM :
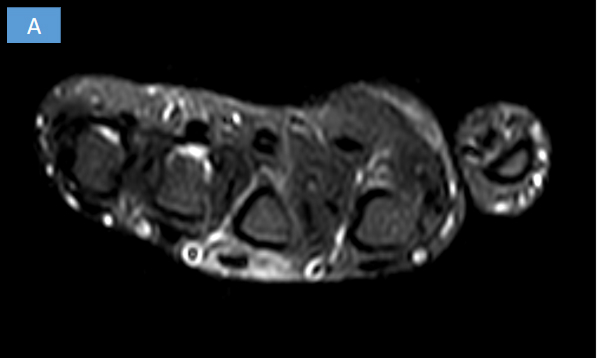
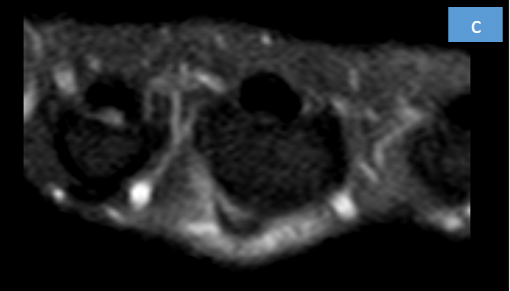
- There is ulnarward subluxation of the extensor digitorum tendon of the middle finger at the level of metacarpophalangeal joint.
- Mild edema seen in the surrounding soft tissue.
- Defect/tear in the sagittal band of the extensor hood of the right middle finger.
- Mild intrasubstance STIR hyperintensity within the extensor digitorum tendon, suggesting tendinosis.
Tendinosis and ulnarward subluxation of extensor digitorum tendon of right middle finger at the level of metacarpophalangeal joint with defect/tear in the sagittal band of the extensor hood.
- Tendinosis of the extensor digitorum tendon at the metacarpophalangeal (MCP) joint could result from injury or chronic degenerative condition.
- At the level of the MCP joint, stability of the extensor digitorum tendon is maintained by the sagittal bands, which are critical components of the extensor hood mechanism.
- A defect or tear in the sagittal band—most commonly involving the radial sagittal band—results in loss of centralization of the extensor tendon over the metacarpal head. This predisposes the tendon to ulnarward subluxation, particularly during MCP joint flexion.
- The middle finger is especially vulnerable due to increased biomechanical forces and relative weakness of the stabilizing structures.
- Sagittal band injury may be traumatic (e.g., direct blow, forceful flexion) or attritional, often associated with repetitive stress, inflammatory arthropathies, or chronic tendon degeneration.
- Clinically, patients may present with pain, snapping, tendon instability and difficulty initiating MCP joint extension.
Magnetic Resonance Imaging (MRI)
- Increased intratendinous signal intensity on T1- and T2-weighted or PD fat-suppressed sequences indicating tendinosis
- Focal discontinuity or thinning of the sagittal band at the MCP joint
- Ulnar displacement of the extensor digitorum tendon relative to the metacarpal head
- Peritendinous edema and soft tissue inflammation
- Absence of complete tendon rupture
- MRI is particularly useful for assessing the integrity of the extensor hood, characterizing chronicity, and evaluating associated soft tissue abnormalities.
DIFFERENTIAL DIAGNOSES :
- Sagittal band rupture without tendon degeneration
- Extensor tendon tenosynovitis
- Rheumatoid arthritis–related extensor tendon instability
- Traumatic extensor tendon tear at the MCP joint
- Trigger finger (stenosing tenosynovitis)
- MCP joint collateral ligament injury
- Ganglion cyst causing mechanical tendon displacement
References
- Wolfe SW, Hotchkiss RN, Pederson WC, Kozin SH. Green’s Operative Hand Surgery. 7th ed. Elsevier; 2017.
- Bianchi S, Martinoli C. Ultrasound of the Musculoskeletal System. Springer; 2007.
- Magee T. MRI of sagittal band injuries of the metacarpophalangeal joint. AJR Am J Roentgenol. 2009;193(1):W28–W33.
- Rayan GM, Murray D. Classification and treatment of closed sagittal band injuries. J Hand Surg Am. 1994;19(4):590–594.
- Schweitzer ME, Karasick D. MR imaging of disorders of the extensor mechanism of the hand. Radiol Clin North Am. 2006;44(4):625–637.
Dr ASHWINI C
MD, FRCR
Consultant - Manipal Hospitals, Hebbal
Dr S Shreya
MBBS, MD
Cross section imaging fellow - MHRG
